Addressing SDOH in FQHCs: A Data-Driven Approach to Better Patient Outcomes
Posted on :
Apr 14, 2025
Introduction
Federally Qualified Health Centers (FQHCs) play a crucial role in the American healthcare system, serving as a lifeline for underserved and vulnerable populations. With over 30 million Americans relying on FQHCs for primary care annually (HRSA, 2023), these centers are at the forefront of community health. Yet, their ability to deliver impactful care is increasingly challenged by the social determinants of health (SDOH)—non-medical factors that significantly influence health outcomes.
More than 1 in 10 patients at FQHCs face major SDOH-related barriers such as housing instability, food insecurity, lack of transportation, and financial strain (JAMA Internal Medicine, 2022). These risk factors are not just background noise—they are the root causes of poor adherence, chronic disease progression, missed appointments, and increased hospitalizations.
This blog expands on our earlier FQHC guide and offers a deeper dive into how SDOH impacts care delivery—and how FQHCs can adopt a structured, data-informed approach to care management that bridges clinical and social care.

What Are Social Determinants of Health (SDOH)?
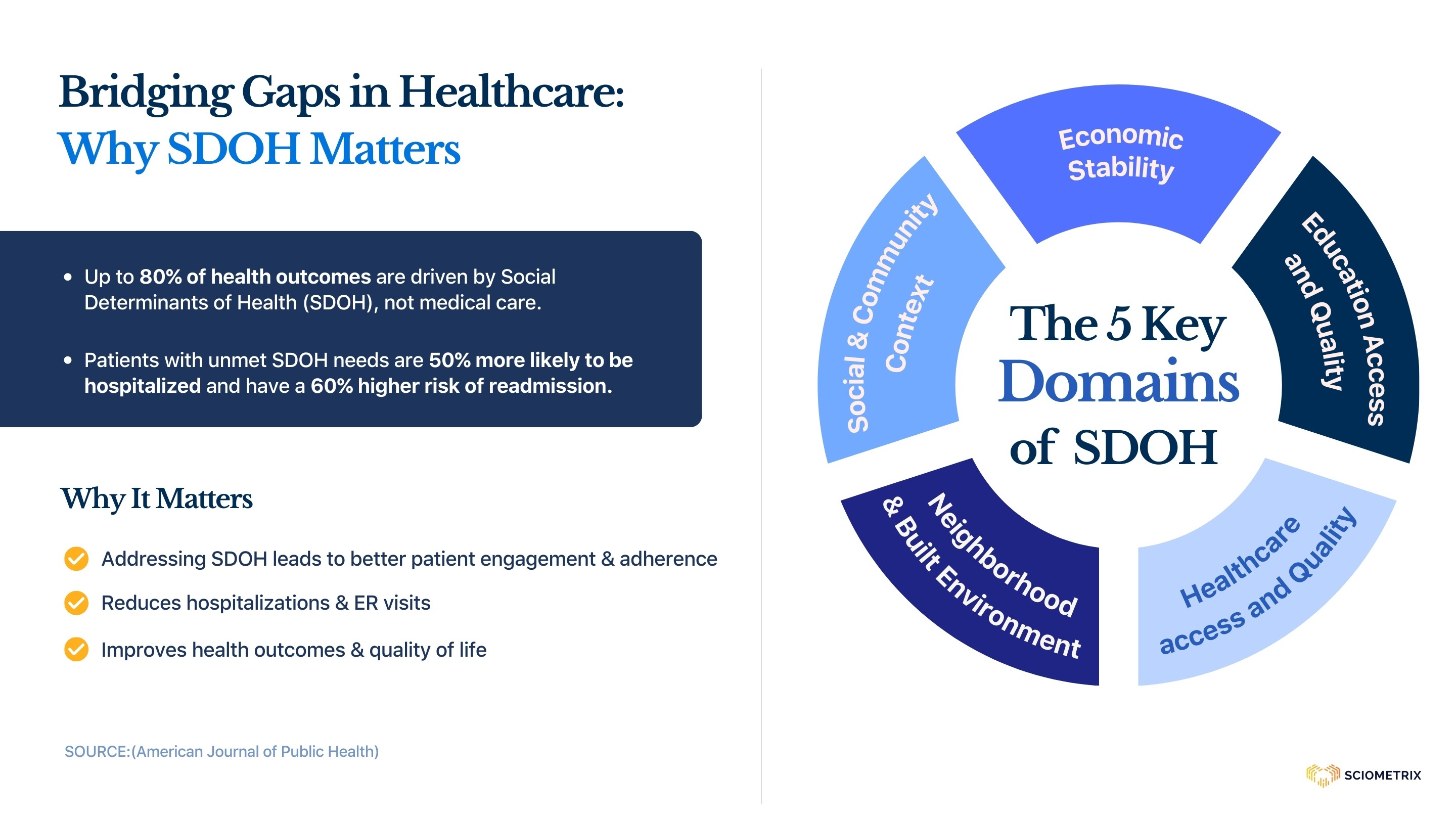
According to the World Health Organization, SDOH are the conditions in which people are born, grow, live, work, and age. The CDC classifies SDOH into five key domains:
1) Economic Stability – Employment, income, expenses, debt, medical bills
2) Education Access and Quality – Literacy, language, early childhood education
3) Healthcare Access and Quality – Health coverage, access to care, provider bias
4) Neighborhood and Built Environment – Housing, transportation, safety, walkability
5) Social and Community Context – Social integration, support systems, discrimination
When these domains are compromised, even the best clinical interventions can fall short.

Bridging the Gap Between Clinical and Social Care
FQHCs are uniquely positioned to close the gap between clinical needs and social realities. But doing so effectively requires more than goodwill—it demands infrastructure, intention, and innovation. To bridge this gap, FQHCs must:
Acknowledge SDOH as Clinical Risk Factors: Treat social needs as core components of the care plan—not as external issues.
Empower the Care Team: Equip staff with tools and training to identify and respond to non-clinical barriers.
Embed SDOH Data into Workflows: Integrate screening and documentation directly into EHR systems and daily care routines.
By shifting from reactive care to proactive, personalized interventions that consider social context, FQHCs can dramatically improve long-term outcomes for their patients.
Why FQHCs Need to Address SDOH Proactively
FQHCs serve communities where SDOH-related challenges are the norm, not the exception. Left unaddressed, these barriers drive up healthcare costs, reduce provider productivity, and worsen patient outcomes.
Addressing SDOH is not an add-on; it’s central to mission-driven, value-based care. Incorporating SDOH data into care planning allows providers to:
Tailor interventions to each patient’s reality
Improve medication and care plan adherence
Prevent avoidable ED visits and readmissions
Increase patient satisfaction and trust
Solutions: What FQHCs Can Do Today
Screen for SDOH Systematically
Use standardized tools like PRAPARE, AHC-HRSN, or the CMS SDOH ICD-10 Z codes
Embed SDOH screening into intake workflows
Train staff to ask sensitive questions with empathy and cultural competence
Build Partnerships with Community-Based Organizations (CBOs)
Refer patients to housing services, food pantries, transit assistance
Establish closed-loop referral systems that track follow-ups
Apply for HRSA or CDC grants to fund local partnerships
Implement a Tech-Enabled Care Management Model
Use EHR-integrated platforms to track SDOH and risk stratify patients
Deploy multilingual RNs for patient outreach and education
Utilize care coordination dashboards for follow-ups, flags, and escalations
Partner with specialized care management companies that offer end-to-end support—from SDOH screenings and resource referrals to continuous patient follow-up—so your team can focus on clinical excellence while extending their reach into the community
Leverage Value-Based Payment Models
Many state Medicaid programs offer SDOH-related incentives under Managed Care Organizations (MCOs)
Participate in CMS programs like ACO REACH, CHART Model, or Community Health Access and Rural Transformation
5. Monitor and Share Data Outcomes
Report improvements in hospitalization rates, patient-reported outcomes, and cost savings
Use data insights to apply for funding and scale successful programs
How Sciometrix Helps FQHCs Address SDOH?
At Sciometrix, we understand that SDOH data isn’t just information—it’s a call to action. We deliver care management services like Chronic Care Management (CCM) and Remote Patient Monitoring (RPM). Our platform is built to bridge the clinical-social care divide:
Risk Stratification Built into Workflows – Our system flags patients with high social risk automatically
US-Based RN Outreach – Our nurses assess and follow up on SDOH in real-time Community
Resource Integration – Our platform connects with CBOs to close the loop Multilingual,
Culturally Sensitive Support – Because equity starts with access
Data Reporting for Grant and Compliance Needs – Supporting your funding and policy efforts

Conclusion: Leading the Future of Community Health
Addressing SDOH isn’t a luxury—it’s a necessity for FQHCs to thrive in a value-based world. Through structured programs, data-driven tools, and community partnerships, FQHCs can overcome systemic barriers and provide transformative care.
At Sciometrix, we are proud to be a trusted partner in this journey. Together, we can move the needle on care delivery—one patient, one intervention, one community at a time.